
There is a conversation happening across cardiology clinics, social media threads, and family WhatsApp groups that was almost unheard of a decade ago. People are asking their doctors about lipoprotein(a), apolipoprotein B, and high-sensitivity C-reactive protein. Terms that once lived exclusively in research papers are now being discussed at the dinner table, and for good reason.
This shift is not driven by a new fad. It is driven by a growing recognition that the standard lipid panel, the one that measures total cholesterol, LDL, HDL, and triglycerides, tells an incomplete story. For Indians and other South Asians in particular, that incomplete story has consequences. The median age for a first heart attack in South Asians is approximately 53 years, compared to 63 years in Western European populations, according to the INTERHEART study. That is a full decade earlier. Understanding why requires looking beyond LDL cholesterol, and that is precisely where Lp(a), ApoB, and hsCRP come in.
The standard lipid panel was designed to be simple, accessible, and broadly applicable. In many ways, it succeeds at all three. But simplicity comes at a cost.
LDL cholesterol, the so-called “bad” cholesterol, measures the total amount of cholesterol carried inside LDL particles. What it does not tell you is how many of those particles are circulating in your blood, how large or small they are, or whether there are other atherogenic (plaque-forming) particles present that carry no cholesterol at all. It also cannot detect certain inherited conditions that raise cardiovascular risk independently of LDL.
For a population that develops coronary artery disease earlier and more aggressively than most others in the world, relying solely on LDL cholesterol is a bit like measuring a building’s fire risk by looking only at the number of rooms. The number matters, but it is not the whole picture.
Lipoprotein(a), written as Lp(a) and pronounced “LP little a,” is a particle that resembles LDL in structure but carries an additional protein called apolipoprotein(a) wrapped around it. This structural difference makes it particularly dangerous. Lp(a) is atherogenic, pro-inflammatory, and anti-fibrinolytic, meaning it promotes plaque formation, drives arterial inflammation, and interferes with the body’s ability to dissolve blood clots.
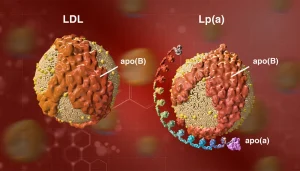
What makes Lp(a) exceptional is that its level in the blood is almost entirely determined by genetics. Diet, exercise, and statins have very little effect on it. You are essentially born with a set Lp(a) level, and it remains relatively stable throughout your life. This means it needs to be measured only once, but it also means there is no lifestyle intervention that will meaningfully lower it.
Elevated Lp(a) is defined differently by different guidelines, but a level above 50 mg/dL (or approximately 125 nmol/L) is generally considered high risk. Here is the critical point for South Asians: approximately 25% of Indians have elevated Lp(a) levels, and research suggests that this higher prevalence may be one contributing factor to the earlier and more aggressive onset of coronary artery disease in this population. A 2020 systematic review published in PubMed (PMID 32295712) specifically examined elevated Lp(a) in South Asians and its association with cardiovascular disease risk.
Lp(a) contributes to risk through multiple pathways simultaneously: it accelerates atherosclerosis, promotes inflammation within arterial walls, and impairs fibrinolysis. For a young person with a normal LDL who has a heart attack, elevated Lp(a) is very often found to be the silent culprit.
What you need to know: Lp(a) is measured with a simple blood test and needs to be done only once in adulthood. If it is elevated, it changes the risk conversation significantly, even if your LDL appears normal. There are no currently approved pharmacological treatments specifically for Lp(a) reduction in India at the time of writing, but knowing your level allows for more aggressive management of other modifiable risk factors.
To understand ApoB, it helps to understand what LDL cholesterol actually measures. LDL-C is a measure of the amount of cholesterol packed inside LDL particles. It tells you about the cargo, not the vehicles carrying it.
ApoB, or apolipoprotein B-100, is a protein that sits on the surface of every atherogenic lipoprotein particle, including LDL, VLDL, IDL, and lipoprotein(a). Crucially, each of these particles carries exactly one ApoB molecule. This means that an ApoB measurement gives you a direct count of the total number of atherogenic particles circulating in your blood.
Why does this matter? Because cardiovascular risk is driven more by the number of atherogenic particles than by the amount of cholesterol they carry. Two people can have identical LDL-C levels but very different ApoB concentrations. The person with more ApoB has more particles attempting to cross the arterial wall and initiate plaque formation, and therefore a higher risk.
This phenomenon of discordance between LDL-C and ApoB is particularly relevant for people with insulin resistance, metabolic syndrome, or elevated triglycerides, all conditions that are disproportionately prevalent in South Asians. In these individuals, LDL particles tend to be smaller and denser, meaning more particles are needed to carry the same cholesterol load. Their LDL-C may look acceptable, but their particle count, and therefore their ApoB, can be significantly elevated.
A large study using UK Biobank data (published in PubMed, PMID 40887080) found that ApoB outperformed LDL particle number as a marker of cardiovascular risk. The European Society of Cardiology and the European Atherosclerosis Society have both stated that ApoB is a more accurate marker of cardiovascular risk than LDL-C. The Lipid Association of India also recognises ApoB as a useful metric in risk assessment.
What you need to know: ApoB is measured with a fasting blood test. An ApoB level below 80 mg/dL is generally targeted for high-risk individuals, though reference ranges vary by guideline. If your LDL looks normal but your ApoB is elevated, the latter is the more meaningful number for cardiovascular risk.
The third piece of this puzzle is hsCRP, or high-sensitivity C-reactive protein. CRP is a protein produced by the liver in response to inflammation. The “high-sensitivity” version of the test detects very low concentrations of CRP, the kind associated with chronic, smouldering inflammation rather than acute infection.
Why does this matter for heart disease? Because atherosclerosis, the process of plaque building up in arterial walls, is not purely a problem of lipid accumulation. It is also an inflammatory process. Plaque formation involves immune cell infiltration, oxidative stress, and a sustained low-grade inflammatory environment within the arterial wall. hsCRP is a measurable reflection of this systemic inflammatory state.
Large prospective studies, including one published in the New England Journal of Medicine (PMID refers to the landmark Women’s Health Study), found that hsCRP was a strong independent predictor of future myocardial infarction, stroke, and vascular death, even among individuals without prior cardiovascular disease.
For Indians, this biomarker carries particular relevance. Research has consistently shown that South Asians have higher hsCRP levels than European populations, even after adjusting for known risk factors. Data from the Chennai Urban Rural Epidemiology Study (CURES-105, published in PMC3192605) found that elevated hsCRP, along with other inflammatory cytokines, was significantly associated with metabolic syndrome and insulin resistance in Asian Indians. Separately, a study on Asian Indians living in the United States (PMID 12915668) found that they had elevated plasma hsCRP concentrations compared to matched non-South-Asian controls.
The Lipid Association of India guidelines identify hsCRP greater than 2 mg/L as a risk modifier, meaning it can tip the decision towards initiating or intensifying lipid-lowering therapy in patients who sit in an intermediate risk category.
Risk interpretation for hsCRP generally follows these thresholds:
What you need to know: hsCRP is a fasting or non-fasting blood test. An elevated result prompts two questions: what is driving the inflammation, and how aggressively should cardiovascular risk be managed? It is best interpreted alongside lipid markers, not in isolation.
Each of these biomarkers reveals something the standard lipid panel cannot. Lp(a) identifies an inherited, independent risk that sits outside the usual risk factor framework. ApoB corrects for the inaccuracies of LDL-C, especially in people with insulin resistance or metabolic syndrome. hsCRP adds the inflammatory dimension, which is increasingly understood to be a core driver of atherosclerotic disease.
In a population where heart attacks occur a decade earlier than expected, where the phenotype of cardiovascular disease is often more aggressive, and where metabolic syndrome and central adiposity are common even in people of normal weight by conventional BMI standards, relying on total cholesterol and LDL alone is genuinely insufficient.
The conversation around these markers is not about anxious over-investigation. It is about precision. A person who knows that their Lp(a) is elevated, their ApoB is high despite a normal LDL, and their hsCRP reflects chronic inflammation, is in a position to make genuinely informed decisions about risk management, in collaboration with their physician.
The first step is simply to have an informed conversation with your doctor. Not every person needs all three tests at every health check. But understanding what these markers are, what they measure, and why they matter for South Asians is a reasonable starting point.
If you have a personal or family history of premature heart disease (defined broadly as a first cardiac event before age 55 in a male first-degree relative or before age 65 in a female first-degree relative), or if you have metabolic syndrome, diabetes, or persistent cardiovascular risk despite apparently normal cholesterol levels, asking about Lp(a), ApoB, and hsCRP is a clinically reasonable request.
The science on these markers has matured considerably. The testing is available, the evidence is robust, and the clinical guidelines are catching up. The real question is not whether these markers matter. It is whether we are asking about them.
To know more about advanced tests that can determine your health risk, take our smart health screener quiz: https://www.vitalishealth.in/smart-whole-body-checkup/